 Have you been told that you — or someone important to you — has heart failure?
Have you been told that you — or someone important to you — has heart failure?
This wouldn’t surprise me, as this is one of the most common heart conditions affecting older adults. People are sometimes alarmed by the term “heart failure”; does it mean the heart is about to stop working? Luckily, that’s not usually the case.
Heart failure actually means that the heart is not pumping or filling as well as it should. This can affect how well blood moves through the body, and it can lead to symptoms such as shortness of breath, fatigue, swelling, and reduced ability to exercise.
Heart failure can be serious, and it is important to take it seriously. But it is also a condition that many older adults live with for years, especially when it is properly diagnosed and treated.
In this article, I’ll explain:
- What heart failure means
- The main types of heart failure
- Common causes in older adults
- Symptoms to watch for
- How heart failure is diagnosed
- How it is treated and managed
- What to know if an older person is frail
- Questions to ask the doctor
This information is based on a Better Health While Aging video podcast conversation with cardiologist Cara Pellegrini, MD, who is a professor at UCSF.
What Is Heart Failure?
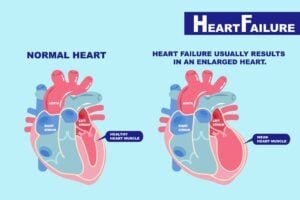
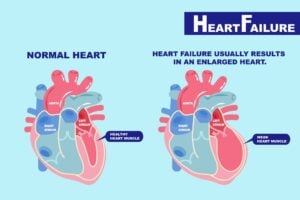
Heart failure means that the heart is experiencing some level of dysfunction in its ability to pump blood to meet the needs of the body.
How the heart works
The heart’s job is to move blood through the body. Veins bring the blood back to the heart, into the right side, from which blood is sent to the lungs to release carbon dioxide and pick up oxygen. From the lungs, the blood returns to the left side of the heart and from there, the left ventricle — the heart’s main pumping chamber — pushes oxygen-rich blood out to the rest of the body.
With each heartbeat, the heart alternates between two states:
- Systole is when the heart squeezes to empty the ventricles and pump blood
- Diastole is when the heart relaxes to fill the ventricles with blood
When the heart is not pumping as efficiently as it should, the body may not get enough blood flow. In some people, fluid can also build up in the lungs, legs, or abdomen.
This is why heart failure used to often be called “congestive heart failure.” The word “congestive” refers to the extra fluid that can accumulate when the heart and kidneys are trying to compensate for reduced blood flow. However, not everyone with heart failure has obvious congestion, so many clinicians now simply use the term “heart failure.”
The Two Main Types of Heart Failure
Most heart failure affects the left side of the heart. There are two main types:
- Systolic heart failure: the heart has trouble generating a good squeeze to pump the blood forward.
- This can be associated with a dilated or weakened ventricle (the lower heart chamber)
- Diastolic heart failure: the heart has difficulty relaxing and filling with enough blood between beats.
- This often involves a thickened ventricle wall
Two newer terms for heart failure:
In recent years, cardiologists have encouraged health providers to categorize heart failure into these two types:
- Heart failure with reduced ejection fraction, often called HFrEF (pronounced “hef-ref”)
- Heart failure with preserved ejection fraction, often called HFpEF (pronounced “hef-pef”)
Ejection fraction refers to the percentage of blood in the left ventricle that gets pumped out with each beat. It’s usually assessed through an echocardiogram (an ultrasound of the heart).
A normal ejection fraction is usually about 55% or higher. It is not expected to be 100%, because the heart never pumps out all the blood in the ventricle with each beat.
Heart Failure With Reduced Ejection Fraction: HFrEF
This type is often related to systolic dysfunction.
Remember, “systole” refers to the squeezing phase of the heartbeat. In HFrEF, the left ventricle has become weaker and is not squeezing as forcefully as it should.
When the ejection fraction is reduced — for instance 40%, 30%, or lower — this suggests the heart’s squeeze function is impaired.
Heart Failure With Preserved Ejection Fraction: HFpEF
This type is often related to diastolic dysfunction.
“Diastole” refers to the relaxation phase of the heartbeat. During this phase, the heart relaxes and fills with blood.
In HFpEF, the heart may still squeeze well enough for the ejection fraction to look normal. But the heart muscle may be stiff or thickened, making it harder for the ventricle to relax and fill properly.
This is especially common in older adults. Aging itself can be associated with stiffening of the heart and blood vessels, and conditions such as high blood pressure can make this worse over time.
Left-Sided and Right-Sided Heart Failure
Most heart failure involves the left side of the heart, especially the left ventricle. This makes sense because the left ventricle has the demanding job of pumping blood to the entire body.
But some people also have right-sided heart failure, either alone or along with left-sided heart failure. The right side of the heart pumps blood to the lungs. Problems affecting the lungs, heart valves, or right ventricle can contribute to right-sided heart failure.
For most older adults, however, heart failure affects mainly the left ventricle, and the question is whether the person has reduced or preserved ejection fraction.
How Common Is Heart Failure in Older Adults?
Heart failure becomes much more common with age.
It is relatively uncommon in younger adults, but it becomes much more frequent in people over 60 and especially in people in their 70s, 80s, and beyond. The CDC estimates that nearly 6.7 million U.S. adults have heart failure, and population studies show that prevalence rises substantially in later life.
Part of the reason is that, over a lifetime, the heart may be affected by:
- High blood pressure
- Coronary artery disease
- Heart attacks
- Diabetes
- Valve disease
- Arrhythmias, such as atrial fibrillation
- Alcohol or other toxins
- Other metabolic or inflammatory stresses
Even when no single dramatic event has occurred, these cumulative effects can eventually contribute to heart dysfunction.
Common Causes of Heart Failure in Older Adults
Here are the most common causes of heart failure in older adults. Bear in mind that an older person’s heart failure might have several underlying causes.
High Blood Pressure
Longstanding high blood pressure is one of the most common contributors to heart failure in older adults.
When blood pressure is high, the heart has to pump against more resistance. Over time, this can lead to thickening and stiffness of the heart muscle, which is a common pathway to HFpEF. High blood pressure can also contribute to reduced squeeze function in some people.
Coronary Artery Disease and Heart Attacks
The heart muscle needs its own blood supply, delivered through the coronary arteries.
If those arteries become narrowed or blocked, parts of the heart muscle may not get enough oxygen. A complete blockage can cause a heart attack, which may damage the heart muscle and weaken its pumping ability.
Even without a major heart attack, coronary artery disease can contribute to heart dysfunction over time.
Heart Valve Problems
The heart has four main valves that help blood move in the right direction.
Valve problems can contribute to heart failure in two major ways:
- Stenosis, meaning the valve has become narrowed or stiff and does not open well
- Regurgitation, meaning the valve leaks and allows blood to flow backward
In older adults, aortic stenosis is a particularly important valve problem. The aortic valve sits between the left ventricle and the aorta. When it becomes calcified and narrowed, the left ventricle has to work much harder to pump blood out to the body.
Another issue is mitral regurgitation, in which the mitral valve leaks. Sometimes this happens because the left ventricle has become enlarged and stretched, pulling the valve leaflets apart so they no longer close properly.
The good news is that some valve problems now have less invasive treatment options than traditional open-heart surgery, depending on the person’s situation.
Cardiomyopathies
A cardiomyopathy is a problem affecting the heart muscle itself.
Some cardiomyopathies are related to toxins, such as heavy alcohol use over many years. This is important because alcohol-related heart dysfunction can sometimes improve significantly if alcohol is reduced or stopped.
Another condition that is increasingly recognized in older adults is amyloidosis, in which abnormal proteins build up in tissues, including the heart. This can interfere with how the heart muscle works. Newer treatments have made it more important to recognize this condition when it is present.
Arrhythmias
Abnormal heart rhythms can also contribute to heart failure.
Atrial fibrillation, for example, is common in older adults and can worsen heart function, especially if the heart rate is too fast or poorly controlled. Other rhythm problems, such as frequent premature ventricular contractions, can also weaken the heart in some cases.
This is another reason it is important to look for underlying causes. Some rhythm-related causes of heart failure can improve when the rhythm problem is treated.
Diabetes
Diabetes often travels together with other heart failure risk factors.
People with diabetes are more likely to have high blood pressure and coronary artery disease. Diabetes also affects blood vessels and metabolism in ways that can stress the heart.
Good diabetes management can be an important part of protecting heart health.
Symptoms of Heart Failure in Aging
The most common symptoms of heart failure are:
- Shortness of breath
- Fatigue
- Reduced ability to exercise or do usual activities
- Swelling in the legs, ankles, feet, or abdomen
- Rapid weight gain from fluid retention
Shortness of breath may first show up with exertion, such as walking uphill, climbing stairs, or carrying groceries. As heart failure worsens, a person may become short of breath with less activity.
Some people also notice they feel worse when lying flat. They may need extra pillows or feel more comfortable sleeping propped up. This can happen because fluid backs up into the lungs when lying down.
Other possible symptoms include:
- Chest discomfort
- Lightheadedness
- Feeling unusually weak
- Loss of appetite
- Unexplained weight loss in more advanced heart failure
- Lower blood pressure in some cases
- Higher blood pressure in others, depending on the type and stage
A key point: fatigue and shortness of breath should not automatically be dismissed as “just aging.”
Many older adults assume they are slowing down only because they are older. But sometimes the reason is a treatable medical condition such as heart failure, anemia, lung disease, thyroid disease, or another issue.
Other Conditions That Can Mimic Heart Failure
Heart failure symptoms are important to recognize, but they are not specific enough to diagnose the condition by symptoms alone.
For example, shortness of breath and fatigue can also be caused by:
- Lung disease
- Anemia
- Thyroid problems
- Kidney disease
- Liver disease
- Heart rhythm problems, such as atrial fibrillation
- Coronary artery disease
- Cancer
- Deconditioning
- Medication side effects
Leg swelling is also common in older adults and is often due to venous insufficiency, sometimes called venous stasis. This means the leg veins are not moving blood back up toward the heart as efficiently as they used to. It can cause swelling, but it does not necessarily mean heart failure. You can learn more about it here: Leg Swelling in Aging: What to Know & What to Do.
So if an older person develops swelling, shortness of breath, or fatigue, the right step is not to panic or self-diagnose. The right step is to get a medical evaluation.
How Heart Failure Is Diagnosed
A heart failure evaluation usually starts with a careful history and physical exam.
A health provider should ask about:
- Symptoms, including when they started and what makes them better or worse
- Exercise tolerance
- Weight changes
- Swelling
- Chest pain
- Past heart problems
- Blood pressure
- Diabetes
- Smoking history
- Alcohol use
- Current medications
During the physical exam, the clinician should listen to the heart and lungs, check the legs for swelling, and look at the veins in the neck. The neck veins can sometimes provide clues about whether the body is retaining extra fluid.
Common tests to evaluate heart failure
Electrocardiogram, or ECG/EKG
An ECG checks the electrical activity of the heart. It can show rhythm problems such as atrial fibrillation and may provide clues about prior heart attacks or other heart strain.
Echocardiogram
An echocardiogram is an ultrasound of the heart. This is one of the most important tests when heart failure is suspected.
It will show:
- The ejection fraction
- How well the heart squeezes
- Whether the heart is stiff or thickened
- Whether chambers are enlarged
- How the heart valves are working
- Whether there is fluid around the heart
Chest X-Ray
A chest x-ray can help assess the lungs and may show signs of fluid buildup or other lung problems.
Blood Tests
Blood tests usually include:
- Kidney function
- Electrolytes
- Blood count, to check for anemia
- Thyroid testing, when appropriate
- BNP or NT-proBNP, which can rise when the heart is under stress
Stress Testing or Heart Catheterization
If coronary artery disease is suspected, the clinician may recommend a stress test or, in some situations, a heart catheterization to look directly at the coronary arteries.
Not every person needs every test. The workup should be tailored to the person’s symptoms, health history, and goals.
Does Heart Failure Require Emergency Treatment?
Often no, but sometimes yes; it depends on how severe the symptoms are.
If a person’s symptoms are mild, they can be evaluated and start treatment in an outpatient setting.
Other times, the first presentation of heart failure is more urgent. A person may come to the emergency room very short of breath, with severe fluid overload, low oxygen levels, or other serious symptoms.
Heart failure can also have exacerbations, meaning flare-ups where symptoms suddenly worsen. These may require urgent treatment or hospitalization.
Seek prompt medical help if an older person has:
- New or worsening shortness of breath
- Shortness of breath at rest
- Chest pain
- Fainting
- New confusion with breathing problems
- Rapid weight gain with swelling
- Severe weakness or inability to do usual activities
- Bluish or grayish skin color, depending on skin tone
- Oxygen levels that are low, if being monitored at home
How Severe Is the Heart Failure?
Heart failure severity is often described by how much activity causes symptoms.
A common system for stages of heart failure is the New York Heart Association functional classification:
- Class I: No symptoms with ordinary activity
- Class II: Symptoms with more significant activity, such as hills or stairs
- Class III: Symptoms with mild activity, such as walking short distances or showering
- Class IV: Symptoms even at rest
Clinicians also increasingly think in terms of prevention, and are starting to think of people at high risk of heart failure as “Stage 0 heart failure.” A person with high blood pressure, diabetes, or coronary artery disease may not yet have heart failure, but they are at higher risk and should have those risk factors managed carefully.
This is an important concept: preventing heart failure, or catching it early, is often much easier than treating advanced disease.
How Heart Failure Is Treated and Managed
Heart failure treatment depends on the type, cause, severity, symptoms, and the older person’s overall health and goals.
The main pillars are:
- Treat reversible causes when possible
- Manage contributing conditions
- Use appropriate heart failure medications
- Support healthy lifestyle habits
- Monitor symptoms and fluid status
- Consider procedures or devices when appropriate
- Match treatment to the person’s goals of care
Treating the Underlying Cause
Treatment should begin with understanding what caused or contributed to the heart failure.
Depending on the situation, this may mean:
- Treating high blood pressure
- Reducing or stopping alcohol
- Managing diabetes
- Treating coronary artery disease
- Treating atrial fibrillation or other arrhythmias
- Evaluating and treating valve disease
- Reviewing medications that may worsen heart failure
- Considering less common causes, such as amyloidosis
This is why it is so important to ask: “What do you think caused this, and can any part of it be reversed?”
Lifestyle and Cardiac Rehabilitation
For most people with heart failure, lifestyle changes can help support the heart and improve quality of life.
Reducing or avoiding alcohol, in particular
These often include:
- Avoiding excessive alcohol
- Staying physically active within safe limits
- Quitting smoking
- Managing weight
- Eating in a heart-healthy way
- Following individualized advice about salt and fluid intake
Some people benefit from cardiac rehabilitation, a supervised exercise and education program. This can be especially helpful after a hospitalization or when a person needs support safely rebuilding endurance.
Salt and Fluid Intake
For people who retain fluid, reducing sodium can help prevent congestion and swelling.
Some people may also be advised to limit fluid intake, but this is not appropriate for everyone. Older adults can be vulnerable to dehydration, kidney problems, and medication side effects, so fluid advice should be individualized.
It’s best to ask the clinician:
“Should I be limiting salt or fluids, and if so, what specific limits do you recommend for me?”
Medications to Treat Heart Failure
Medications are often extremely helpful in heart failure. In some areas of medicine, we worry about too many medications, especially in older adults. But for heart failure, several medication classes have strong evidence showing they can improve symptoms, reduce hospitalizations, and help people live longer.
Medications for HFrEF (systolic heart failure)
Current American Heart Association guidance recommends four core medication classes for heart failure with reduced ejection fraction:
- Beta Blockers
- Examples include carvedilol and metoprolol
- Beta blockers slow the heart rate and reduce the heart’s workload. They can help the heart function more efficiently over time.
- ACE Inhibitors, ARBs, or ARNI
- Examples include lisinopril and valsartan
- These medications help relax blood vessels and influence hormone systems related to blood pressure, salt, and fluid balance.
- An ARNI is a newer combination medication that includes sacubitril and valsartan. It is often used in people with HFrEF when appropriate.
- Mineralocorticoid Receptor Antagonists, or MRAs
- Examples include spironolactone and eplerenone
- MRAs are gentle diuretics that also affect hormone pathways involved in heart failure. They can help with fluid balance and potassium regulation, but kidney function and potassium levels must be monitored.
- SGLT2 Inhibitors
- Examples include empagliflozin and canagliflozin
- SGLT2 inhibitors were originally developed for diabetes, but they have also been shown to help many people with heart failure, even those without diabetes.
Diuretics
Many people with heart failure also need a diuretic, sometimes called a water pill. These medications help the body get rid of extra fluid and can quickly improve symptoms such as swelling and shortness of breath. Furosemide (brand name Lasix) is a common diuretic used for heart failure.
Medications for HFpEF (diastolic dysfunction)
For heart failure with preserved ejection fraction, treatment has historically been more challenging. However, newer evidence has shown benefits from some of the same medication classes, especially in certain patients.
Treatment may include:
- SGLT2 inhibitors
- MRAs
- ARNI or related blood-pressure medications in selected cases
- Diuretics for fluid overload
- Careful blood pressure control
- Management of atrial fibrillation, diabetes, kidney disease, and obesity when present
Because HFpEF is common in older adults and often coexists with several other conditions, treatment needs to be individualized.
Self-Monitoring at Home
For many people with heart failure, self-monitoring can help prevent hospitalizations.
A common recommendation is to weigh yourself every day, ideally at the same time each morning. A rapid increase in weight can mean fluid is building up.
Ask the doctor what specific change should trigger a call. Many clinicians use a threshold such as several pounds over a day or two, but the exact recommendation may vary.
It can also be helpful to monitor:
- Shortness of breath
- Swelling
- Ability to do usual activities
- Blood pressure, if recommended
- Heart rate, if recommended
- Dizziness or falls
- Medication side effects
The key is to notice early worsening before it becomes severe.
Useful questions include:
- “Should I weigh myself every day?”
- “How much weight gain should prompt me to call?”
- “Should I monitor my blood pressure?”
- “What symptoms mean I should seek urgent care?”
- “Do I have a plan for adjusting my diuretic if my weight goes up?”
Heart Failure Treatment in Frail Older Adults
Older adults, especially those who are frail, often need extra care when treating heart failure.
They may be more sensitive to:
- Blood pressure drops
- Dizziness
- Falls
- Kidney function changes
- Electrolyte problems
- Medication side effects
- Dehydration
This does not mean they should not receive treatment. It means treatment should be thoughtful, monitored, and aligned with what matters most to the person.
For instance, a frail older adult may still benefit greatly from medications that improve breathing and energy. But doses may need to be started low and adjusted carefully.
It’s also important not to dismiss symptoms as “just aging.” Shortness of breath, fatigue, reduced activity, and swelling deserve evaluation, even in very old adults.
At the same time, goals of care matter. Some people want all reasonable treatments that might extend life. Others want to focus more on comfort, function, and avoiding burdensome procedures. Many people want both: to live longer if possible, but not at the cost of unacceptable side effects or loss of quality of life.
Good care requires talking through these tradeoffs.
Procedures and Devices Used in Heart Failure
Some people with heart failure may benefit from procedures or implanted devices.
Treating Valve Disease
If a valve problem is a major contributor, treating the valve may improve symptoms and heart function.
For example, severe aortic stenosis can sometimes be treated with a catheter-based procedure rather than open-heart surgery, depending on the person’s situation.
Mitral regurgitation may also have catheter-based treatment options in selected cases.
Biventricular Pacemaker
A biventricular pacemaker, also called cardiac resynchronization therapy, can help certain people who have systolic dysfunction with an ejection fraction less than 35%.
This device helps coordinate the heart’s contractions. In the right person, it can really improve symptoms, as well as help people live longer.
Implantable Cardioverter-Defibrillator, or ICD
An ICD watches the heart rhythm and can deliver a shock if a life-threatening rhythm occurs.
This device is mainly focused on preventing sudden cardiac death in people at higher risk, such as those with a very low ejection fraction or a history of dangerous arrhythmias.
For older adults, especially those with serious frailty or advanced illness, it is important to discuss whether an ICD fits their goals. Some people want this protection. Others may decide that if their heart develops a sudden fatal rhythm, they would not want to be shocked back.
For people who already have an ICD, it is also possible to discuss turning off the shock function later in life if goals change.
Heart Failure, Atrial Fibrillation, and Arrhythmias
Atrial fibrillation is a common heart rhythm problem in older adults. It can coexist with heart failure and sometimes worsen it.
When atrial fibrillation causes the heart to beat too fast or irregularly for long periods, it can contribute to worsening heart function. Treating atrial fibrillation may improve symptoms and, in some cases, heart function.
Other rhythm issues, such as frequent premature ventricular contractions, can also contribute to heart dysfunction in selected patients.
This is one reason an ECG and sometimes longer rhythm monitoring may be recommended.
For more on atrial fibrillation: Atrial Fibrillation in Aging: What to Know & How to Treat.
Can People Die of Heart Failure?
Yes, heart failure can be life-limiting, especially when it becomes advanced.
However, many people with heart failure live for years, and many die of something else. Prognosis depends on the cause, severity, response to treatment, age, other medical conditions, and overall resilience.
When heart failure does contribute to death, it may happen in different ways:
- Sudden cardiac death from a dangerous rhythm
- Heart attack
- Gradual worsening of pump function
- Progressive weakness, weight loss, and reduced function
- Repeated hospitalizations and complications
For advanced heart failure, palliative care can be very helpful. Palliative care focuses on symptom relief, decision-making support, and quality of life. Hospice may also be appropriate when heart failure is advanced enough and the focus has shifted to comfort.
These services do not mean “giving up.” They can help people live as well as possible with serious illness.
Questions to Ask the Doctor About Heart Failure
If you or an older loved one has been diagnosed with heart failure, consider asking:
- What type of heart failure do I have?
Is it heart failure with reduced ejection fraction, preserved ejection fraction, or something else? Is it only on the left side, or is the right side of the heart affected as well? - What is my ejection fraction?
What did the echocardiogram show? - What do you think caused my heart failure?
Could it be related to blood pressure, coronary artery disease, valve disease, atrial fibrillation, alcohol, amyloidosis, or something else? - Are any causes reversible or treatable?
- How severe is my heart failure?
What level of activity should I be able to do? - What medications do you recommend, and why?
- What side effects should I watch for?
- Do I need to monitor my weight, blood pressure, or heart rate at home?
- How much weight gain should prompt a call?
- Should I limit salt or fluids? If so, how much?
- Would cardiac rehabilitation help me?
- Do I need to see a cardiologist or heart failure specialist?
- Are there any procedures or devices I should consider?
- How do these treatment options fit with my goals of care?
The Bottom Line
Heart failure is common in older adults, but it does not mean the heart has completely failed or that death is imminent.
It usually means the heart is not pumping or filling as well as it should. The most common symptoms are shortness of breath, fatigue, reduced exercise tolerance, swelling, and rapid weight gain from fluid.
Because these symptoms can also be caused by other conditions, it is important to get a medical evaluation rather than self-diagnosing.
The good news is that heart failure is often very treatable. Many people feel better with the right medications, lifestyle support, monitoring, and treatment of underlying causes. Some people even have improvement in heart function, especially when a reversible contributor is found.
For older adults and families, the most important steps are to understand the type of heart failure, ask what may have caused it, learn how to monitor symptoms, and make sure treatment decisions are aligned with the older person’s health priorities and goals.